
Why Inflammation Does Not Always Show Up on Standard Blood Tests
Inflammation is increasingly recognised as an important contributor to many persistent pain conditions. However, one of the most common misconceptions in healthcare is that normal routine blood tests necessarily exclude the presence of ongoing inflammatory or immune-related dysfunction.
Standard inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are highly useful for detecting significant systemic inflammation, infection, or autoimmune disease. However, these markers may remain within normal ranges despite the presence of more subtle neuroimmune and low-grade inflammatory processes associated with chronic pain states (Kosek et al., 2016).
Contemporary research has demonstrated that persistent pain can involve complex interactions between the nervous system and immune system, including altered cytokine signalling, glial cell activation, and dysregulated inflammatory responses (Ji et al., 2016). These processes may contribute to heightened nervous system sensitivity without producing abnormalities on routine pathology screening.
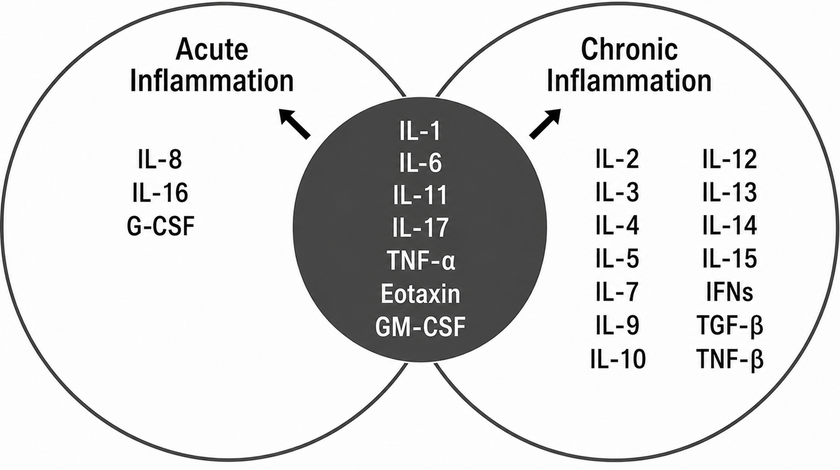
Figure 1. Cytokines involved in acute and chronic inflammatory responses (Feghali & Wright, 1997)
Cytokines are small immune signalling molecules that regulate inflammatory activity throughout the body. Under certain conditions, elevated levels of pro-inflammatory cytokines such as interleukin-6 (IL-6), tumour necrosis factor-alpha (TNF-α), and interleukin-1 beta (IL-1β) may contribute to increased nociceptive sensitivity and amplification of pain processing pathways (Watkins & Maier, 2003; Ji et al., 2016).
Importantly, this does not suggest that all persistent pain is inflammatory in origin, nor that cytokine abnormalities alone explain symptom severity. Contemporary pain science recognises chronic pain as a multidimensional condition influenced by interacting biological, psychological, behavioural, metabolic, and social factors operating simultaneously (Nicholas et al., 2019).
A growing body of evidence nevertheless suggests that low-grade inflammatory activity may be influenced by disrupted sleep, chronic psychological stress, obesity, sedentary behaviour, metabolic dysfunction, and autonomic nervous system dysregulation (Furman et al., 2019). Sleep deprivation in particular has been shown to influence inflammatory signalling pathways and increase pain sensitivity in otherwise healthy individuals (Haack et al., 2020).
These mechanisms may help explain why some individuals continue to experience widespread pain, fatigue, cognitive dysfunction, exercise intolerance, or prolonged recovery despite relatively normal imaging findings and standard laboratory investigations.
Modern pain research increasingly recognises that persistent symptoms may reflect altered physiological regulation rather than isolated structural pathology alone. Consequently, comprehensive assessment may sometimes require consideration of broader neurophysiological, autonomic, metabolic, sleep-related, and inflammatory contributors to symptom persistence.
Importantly, laboratory investigations should never be interpreted in isolation. Blood biomarkers represent only one component of a broader clinical picture and must always be considered alongside clinical history, physical examination findings, functional capacity, sleep quality, stress physiology, movement behaviour, and overall health status.
Contemporary evidence increasingly supports integrated management strategies that combine nervous system regulation, graded rehabilitation, sleep optimisation, physical activity, stress reduction, metabolic health interventions, and patient education as part of long-term pain recovery (Nicholas et al., 2019; Furman et al., 2019).
For individuals experiencing ongoing pain, fatigue, or impaired recovery despite apparently “normal” investigations, a comprehensive systems-based assessment may help identify contributing mechanisms and guide a more targeted management approach.
With kind regards,
Dr. Kevin Ivins
References
Feghali, C. A., & Wright, T. M. (1997). Cytokines in acute and chronic inflammation. Front Biosci, 2(1), d12-d26. https://doi.org/10.2741/A171
Furman, D., Campisi, J., Verdin, E., Carrera-Bastos, P., Targ, S., Franceschi, C., Ferrucci, L., Gilroy, D. W., Fasano, A., Miller, G. W., Miller, A. H., Mantovani, A., Weyand, C. M., Barzilai, N., Goronzy, J. J., Rando, T. A., Effros, R. B., Lucia, A., Kleinstreuer, N., & Slavich, G. M. (2019). Chronic inflammation in the etiology of disease across the life span. Nature Medicine, 25(12), 1822–1832. https://doi.org/10.1038/s41591-019-0675-0
Haack, M., Simpson, N., Sethna, N., Kaur, S., & Mullington, J. (2020). Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology, 45(1), 205–216. https://doi.org/10.1038/s41386-019-0439-z
Ji, R. R., Nackley, A., Huh, Y., Terrando, N., & Maixner, W. (2018). Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology, 129(2), 343–366. https://doi.org/10.1097/ALN.0000000000002130
Kosek, E., Cohen, M., Baron, R., Gebhart, G. F., Mico, J. A., Rice, A. S. C., & Rief, W. (2016). Do we need a third mechanistic descriptor for chronic pain states? Pain, 157(7), 1382–1386. https://doi.org/10.1097/j.pain.0000000000000507
Nicholas, M., Vlaeyen, J. W. S., Rief, W., Barke, A., Aziz, Q., Benoliel, R., Cohen, M., Evers, S., Giamberardino, M. A., Goebel, A., Korwisi, B., Perrot, S., Svensson, P., Wang, S. J., Treede, R. D., & IASP Taskforce for the Classification of Chronic Pain. (2019). The IASP classification of chronic pain for ICD-11: Chronic primary pain. Pain, 160(1), 28–37. https://doi.org/10.1097/j.pain.0000000000001390
Watkins, L. R., & Maier, S. F. (2003). Glia: A novel drug discovery target for clinical pain. Nature Reviews Drug Discovery, 2(12), 973–985. https://doi.org/10.1038/nrd1251