
The Hidden Relationship Between Sleep, Inflammation, and Persistent Pain
Sleep is increasingly recognised as one of the most important biological processes involved in health, recovery, and pain regulation. However, many individuals experiencing persistent pain remain unaware that changes in sleep quality frequently occur long before noticeable worsening of symptoms develops.
Historically, sleep disturbance was often viewed as simply a consequence of pain. Contemporary research now suggests that the relationship is considerably more complex, with growing evidence supporting a bidirectional interaction in which poor sleep may both result from and contribute to persistent pain states (Haack et al., 2019).
Experimental and clinical studies have shown that even relatively modest sleep restriction can increase pain sensitivity and reduce the nervous system's ability to regulate nociceptive input (Chang et al., 2022). Individuals subjected to sleep disruption frequently exhibit lower pain thresholds and heightened responsiveness to sensory stimulation, even among otherwise healthy populations.
One proposed mechanism involves inflammatory signalling pathways. Sleep deprivation has been associated with altered immune activity and increased production of pro-inflammatory cytokines, including interleukin-6 (IL-6) and tumour necrosis factor-alpha (TNF-α), both of which can influence nociceptive processing and nervous system sensitivity (Mullington et al., 2010; Irwin, 2023).
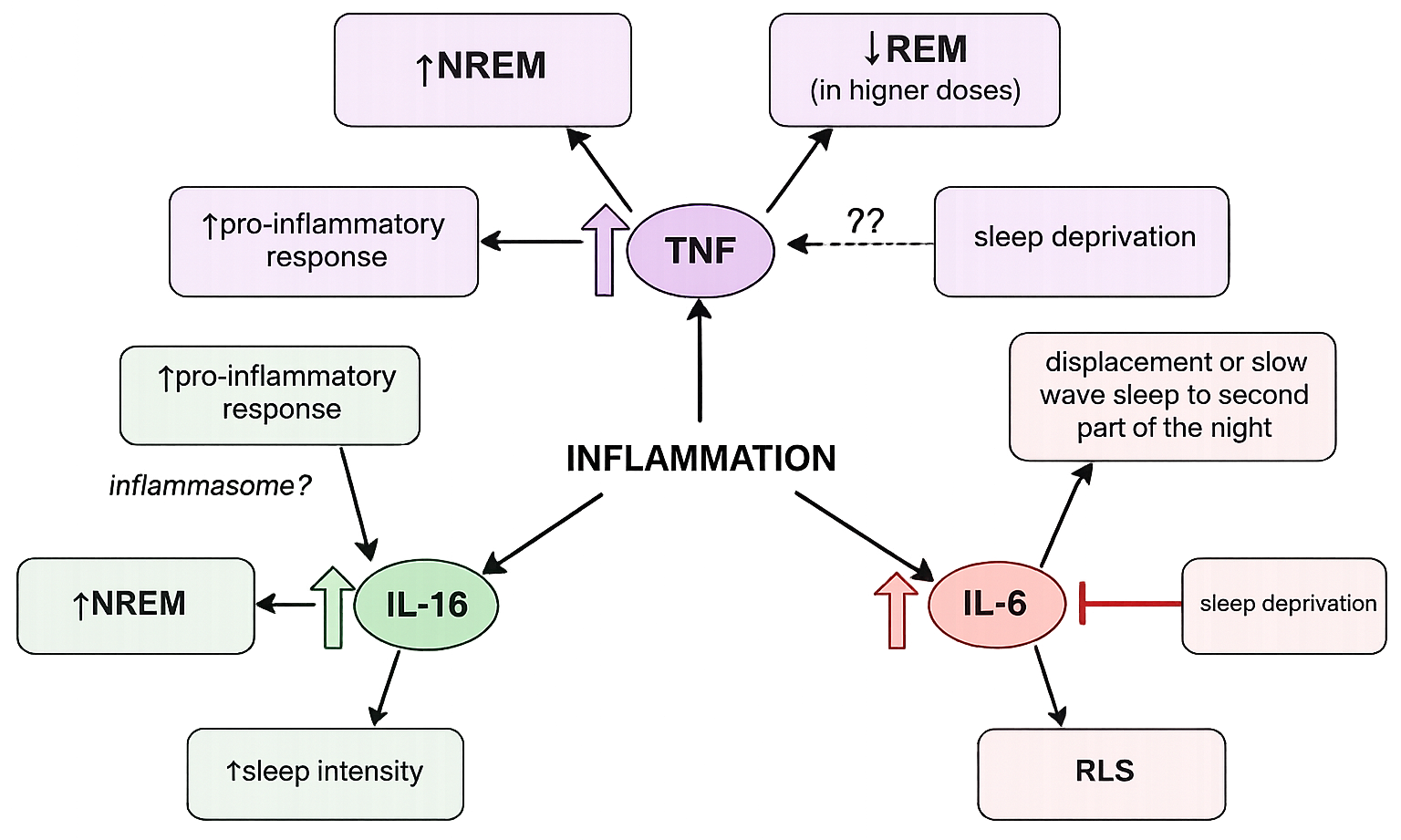
Figure 1. Sleep and inflammation (Ditmer et al., 2021)
Importantly, sleep does not represent a uniform biological state. Different stages of sleep appear to serve distinct physiological functions. Slow-wave sleep, also referred to as deep or N3 sleep, has been associated with restoration, autonomic regulation, and modulation of inflammatory activity, whereas rapid eye movement (REM) sleep contributes to emotional processing, memory consolidation, and adaptive nervous system function (Krueger et al., 2008).
Recent experimental evidence suggests that disruption of slow-wave sleep may contribute to increased inflammatory activation and heightened pain sensitivity, potentially through mechanisms involving immune cell signalling and altered autonomic regulation (Irwin et al., 2023).
Circadian rhythm disruption may also play an important role. The body's internal biological clock coordinates fluctuations in hormone release, immune activity, and sleep architecture across a twenty-four-hour period. Shift work, irregular sleep schedules, prolonged stress exposure, excessive evening light exposure, and inconsistent sleep timing may disturb these regulatory processes and contribute to dysregulated inflammatory signalling (Garbarino et al., 2021).
These interactions may help explain why many individuals with persistent pain report fatigue, non-restorative sleep, reduced recovery capacity, cognitive dysfunction, and progressive worsening of symptoms despite relatively normal imaging or routine investigations.
Modern pain science increasingly recognises sleep as more than a passive period of rest. Sleep represents an active biological process involved in nervous system regulation, tissue repair, immune modulation, and maintenance of physiological resilience.
Consequently, effective long-term pain management may require consideration of sleep quality alongside other contributing factors, including physical activity, stress physiology, autonomic regulation, metabolic health, and broader lifestyle influences.
For individuals experiencing persistent pain, poor sleep quality should not necessarily be viewed as an unrelated symptom. In many cases, it may represent an important component of the overall clinical picture and an opportunity to support recovery.
With kind regards,
Dr. Kevin Ivins
References
Chang, J. R., Fu, S. N., Li, X., Li, S. X., Wang, X., Zhou, Z., Pinto, S. M., Samartzis, D., Karppinen, J., & Wong, A. Y. (2022). The differential effects of sleep deprivation on pain perception in individuals with or without chronic pain: A systematic review and meta-analysis. Sleep medicine reviews, 66, 101695. https://doi.org/10.1016/j.smrv.2022.101695
Ditmer, M., Gabryelska, A., Turkiewicz, S., Białasiewicz, P., Małecka-Wojciesko, E., & Sochal, M. (2022). Sleep Problems in Chronic Inflammatory Diseases: Prevalence, Treatment, and New Perspectives: A Narrative Review. Journal of Clinical Medicine, 11(1), 67. https://doi.org/10.3390/jcm11010067
Garbarino, S., Lanteri, P., Durando, P., Magnavita, N., & Sannita, W. G. (2021). Role of sleep deprivation in immune-related disease risk and outcomes. Communications Biology, 4, 1304. https://doi.org/10.1038/s42003-021-02825-4
Haack, M., Simpson, N., Sethna, N., Kaur, S., & Mullington, J. (2019). Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology, 45, 205–216. https://doi.org/10.1038/s41386-019-0439-z
Irwin, M. R., Olmstead, R., Bjurstrom, M. F., Finan, P. H., & Smith, M. T. (2023). Sleep disruption and activation of cellular inflammation mediate heightened pain sensitivity: a randomized clinical trial. Pain, 164(5), 1128–1137. https://doi.org/10.1097/j.pain.0000000000002811
Krueger, J. M., Rector, D. M., Roy, S., Van Dongen, H. P. A., Belenky, G., & Panksepp, J. (2008). Sleep as a fundamental property of neuronal assemblies. Nature Reviews Neuroscience, 9(12), 910–919. https://doi.org/10.1038/nrn2521
Mullington, J. M., Simpson, N. S., Meier-Ewert, H. K., & Haack, M. (2010). Sleep loss and inflammation. Best Practice & Research Clinical Endocrinology & Metabolism, 24(5), 775–784. https://doi.org/10.1016/j.beem.2010.08.014